
Part of the challenge is that MAPs are not a single, standardised technology. Everything from how the drug is delivered – coating, partially or wholly soluble needle, hollow – through needle number – anything from one to thousands – to materials and manufacturing process has been varied and continues to vary. Just like transport has its “last mile” problems and solutions, MAPs have their “last millimetre” problem: how do you get the drug payload from outside the body into the viable layers of the skin in a way which is consistent from person-to-person, day-to-day, and site-to-site?
This is a knotty problem – and one which is, in our experience, often left in the “solve it later” pile. But let’s be straight – this is an unwise approach, and there are many failed MAP projects which evidence this. But it doesn’t have to be that way. A lot of expertise has been built up over the last couple of decades on how to insert MAPs reliably and well. Informed by TTP’s long experience in this space, the purpose of this insight piece is to flag some of the main landmarks to help you navigate through your journey to a successful MAP / inserter system.
What does “successful insertion” mean?
This might sound like a silly question – surely it just means the needles going in? – but it isn’t. What success means depends critically on the nature of the needles, and your delivery constraints.
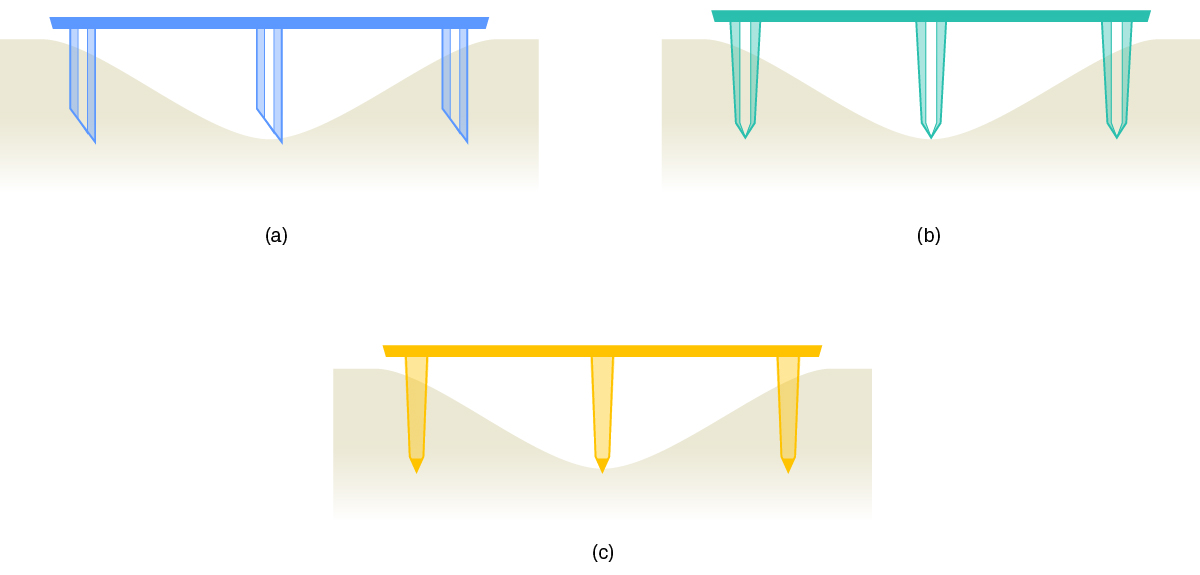
While it would always be ideal to fully insert every needle in a MAP every time, the consequences of imperfect insertion are quite different for different kinds of MAP (figure 1). Since this in turn means that the challenges for an inserter are quite different, it is important for developers to develop individual success criteria before proceeding far with MAP system design.
Hollow microneedles
With hollow microneedles, (figure 1a) each needle has three possible outcomes: (1) it penetrates well, providing a delivery route; (2) it penetrates somewhat, but provides no fluid route; or (3) it doesn’t penetrate, and the lumen is open to the air. Although the ideal is that all needles are type (1), having some type (2) is not a big problem – it just increases the fluid resistance a little. However, if the MAP has any type (3) insertions, it’s all over: the resistance of the path to the floor is much lower than the path to the body, so that’s where the formulation will go. For hollow microneedles, “success” means that most lumens are in the viable skin and all are inserted up to the lumen – and inserting further does not alter drug delivery performance.
Coated microneedles
Drug delivery performance for coated microneedles (figure 1b)is all about the needle area in contact with interstitial fluid. That’s it – inserting any given needle further will increase delivery, and vice versa. This means that the chances of “no dose” are very small, but also that there are no thresholds. For coated microneedles, “success” means repeatable depth of insertion for all needles, and material deviation from this causes significant dose variation.
Soluble microneedles
In many ways, “success” for soluble microneedles is similar to coated, but usually a bit harder. For common, conical microneedles, the area of insertion is proportional to the square of the inserted distance, whereas the inserted volume is in proportion to the cube. This means that a 10% change in insertion depth will give roughly a 20% change in drug delivery for a coated needle, but a 30% change for a soluble one. For soluble microneedles, “success” means repeatable depth of insertion for all needles, and material deviation from this causes very significant dose variation.
Tip-loaded soluble microneedles
More recently, some MAPs are being produced where only the tip contains drug (figure 1c), and the rest of the structure is carrier only. The key difference between this and conventional soluble needles is that, so long as the depth of penetration is great enough that the tips are inserted, drug delivery performance is insensitive to any further penetration. For tip-loaded soluble microneedles, “success” means that the tips penetrate to the viable skin layers – inserting further does not alter drug delivery performance.
Inserter design should therefore be driven by the success criteria for the specific MAP. The question is not simply how to maximise insertion, but how to achieve enough insertion, consistently, for that MAP’s delivery mechanism and the needs of the specific therapy.
Insertion should be as dynamic as necessary… but not more
The go-to method for improving insertion for a MAP is to use an inserter which applies the MAP to the skin at significant speed, as well as controlling the condition of the skin in a variety of different ways. We’ll have more to say on both approaches shortly, but for the moment we’ll consider a more basic question: if dynamic is often better for insertion than static, is more dynamic even better?
In a word, “no” – and for a variety of reasons. The first is simple: being hit hard by an inserter hurts. It’s a different discomfort from a conventional needle for sure, but it is uncomfortable. Other factors, such as the typical whip-crack of the impact, can combine with the sensation to make the experience unsettling. Broadly, the faster the impact, the more significant these effects become, with a notable step up when impact speed exceeds the longitudinal wave propagation speed in subcutaneous tissue (typically 8 m/s to 10 m/s).
Another reason is more technical: higher impact speeds necessarily cause higher amplitude waves to propagate out from the impact site. Longitudinal waves travel directly down into the body, and are partly reflected back at tissue interfaces, most notably when they encounter muscle. We have experience of those reflected waves ejecting a well-installed MAP from the skin entirely – this is not a small effect. Similarly, transverse surface waves will usually encounter the “foot” of the applicator at some point Depending on the geometry, these can also reflect back and converge on the recently-applied MAP.
While these problems can be mitigated to some extent at the expense of a more involved applicator, the best mitigation for any risk is not to take it.
Almost all therapeutic MAPs use dynamic insertion to some extent for increasing and localising contact loads, but it is not a panacea: it should be used as much as is needed, and not more.
Patch mass matters
Needle penetration during dynamic insertion is quite a vigorous process. Primary penetration tends to take place over a few tenths of a millisecond and typically involves accelerations in the region of a few 10⁴ m/s² over a distance of a millimetre or two. This process, and the subsequent few milliseconds of energetic motion, are dominated by inertia and wave propagation as the tissue is accelerated and the MAP slows.
A key consequence is that moving masses are very important, and changing them is likely to alter how penetration works and how successful it is. There are three main contributors to moving mass: the MAP itself, the “plunger” of the applicator, and the spring of the applicator. It is easy to miss some eventual contributors in early testing, so it’s important to watch out for the following.
Will the MAP have a stiff backing or an adhesive film? Is the thickness of the substrate representative?
Does the test plunger have enough material that a latch mechanism could be implemented? A reset (if required)?
Is the same style and mass of applicator spring going to be used? If not, has the effective moving mass been assessed?
Whereas it is typically easier to change the applicator components later, the MAP is often fixed somewhere earlier, so ensuring that all components – or best approximations to all components that have yet to be fixed – are present during testing mitigates the risk of patch mass changing significantly later.
Skin is not flat
We all know that skin is not flat – but skin is not flat in several different ways that matter for MAP insertion.
First, skin has several different kinds of fine lines and wrinkles – not all associated with age – which are typically sub-millimetre in width and depth. Though these are small, they are not necessarily smaller than needle insertion depths, especially in older people: a needle which would have inserted into an idealised “flat” skin might actually remain outside the body.
Second, the act of pushing any sort of applicator tool with an aperture onto the skin will cause some amount of doming. This can have benefits by putting the outer layers of skin into lateral tension, but any doming means that needles near the centre of the MAP will impact before those near the edge. The effect of this can be that the edge needles have a reduced impact speed, and that the domed skin acts like a “stand-off” for the skin at the edge of the dome, holding the needles out.
Last, very few regions of the body are flat to within a microneedle length over distances more than a few centimetres – and those which are flat enough are mostly inaccessible for self-injection. This places a hard-to-change upper limit on the size of a MAP of a few centimetres across.
Although all of these points are familiar, they are frequently neglected when a MAP system is first being considered, leaving a developer with difficult-to-resolve issues later.
Do not assume that near-full penetration is achievable without evidence
It is almost always possible to improve the hand-insertion performance of a MAP with a well-considered applicator – and we have done this for multiple clients. But an inescapable conclusion from this experience is that it is not always possible to achieve full needle penetration with a given MAP – and sometimes very much less than full penetration.
To illustrate this point, consider a finding of ours from some years back.
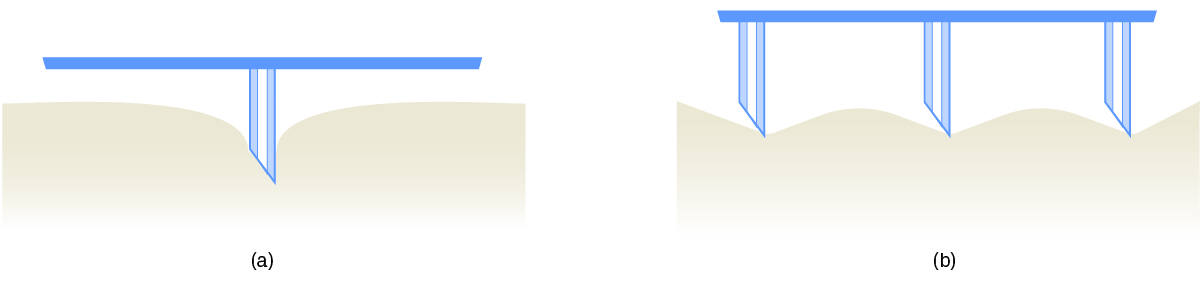
When many individually sharp points are close enough together, the deformations they cause in anything pressed onto them can overlap, resulting in much less penetration than would be otherwise expected – the so-called “bed of nails” effect (figure 2). In a series of experiments, we found that reducing the number of needles on a particular MAP to a quarter of the original barely reduced the number of successful penetrations – and enormously improved repeatability.
The take-home message from this experiment is that achievable delivery can be far less than nominal drug loading. If the MAP modality is selected by an asset team based on nominal loading, and achievable penetration is only checked later, the delivered dose may fall far short of what is needed with very limited options to improve matters.
Our advice is to assess insertion performance early when the MAP design – and preferably even drug concentration – can still be changed. This gives the greatest chance of finding a MAP design and insertion approach which achieve the required drug delivery performance.
About TTP's Drug Delivery team
TTP helps pharma teams turn complex drug delivery challenges into robust, scalable devices ready for clinical and commercial success. Trusted by nine of the top ten global pharmaceutical leaders, our drug delivery product design and development team brings deep design, engineering, scientific and human factors expertise to advanced devices and combination products. We support programmes from early feasibility and concept creation through to verification, transfer to manufacture and launch.
Our experience spans autoinjectors, pens, wearable injectors, inhalation systems, microneedles, implantables and targeted delivery technologies. We help teams retire risks early, resolve trade-offs and address challenges such as high-viscosity biologics, advanced formulations, usability, manufacturability and device reliability. With more than 70 innovative systems developed, TTP brings the technical judgement and multidisciplinary expertise needed to accelerate development and deliver devices that perform in real-world use.
Find out more about our medical device design, human factors and manufacturing expertise.








